This intrigued us since our inclination was to strictly confine our analysis to stay within the boundaries of project data. Although we attempted to use existing conceptual models to structure our understanding and integrate data across the three projects, we ultimately realized that the most salient way to conceptualize this data was by using a theoretical framework. The integrated discussion presented below is predicated on our sense that the most interesting and important contribution of PAHL is less about the specifics of disseminating a school-based obesity prevention intervention in American Indian schools than about what we can learn from the process.
We believe that this integrated, theoretically framed approach provides a novel perspective on the ongoing epistemological debates regarding internal and ecological validity in public health research. Pathways was a large-scale, multi-site randomized control trial RCT funded by the National Heart, Lung, and Blood Institute, to prevent obesity by promoting healthful eating habits and increasing physical activity through a four-component nutrition and physical activity curriculum for elementary schools teaching American Indian children.
The 8-year study, from to , involved 7 Indian Nations, 5 universities including the UNM PRC, and 41 elementary schools with 1, American Indian third- through fifth-grade students Davis et al. Pathways promoted behavioral and environmental approaches to preventing childhood obesity through four, integrated components school curriculum, physical activity enhancements, school food service improvements, and a family component. Although Pathways was an efficacy trial, its design was structured to integrate features that would facilitate translation, including a feasibility study Gittelsohn et al.
Pathways required an extensive formative assessment that was conducted in partnership with tribal communities and was designed to fit these communities Gittelsohn et al. Community members were important contributors to the final form and format of Pathways Davis and Reid Pathways resulted in statistically significant changes in health knowledge, cultural identity, and healthful eating behaviors on the part of third-, fourth-, and fifth-grade school children in comparison to control schools Gittelsohn et al.
Subsequent activity on the Pathways webpage on the site was more extensive than anticipated, and interest from tribes other than those in the original Pathways study and at IHS remained high. Responding to continued interest in Pathways, researchers from the UNM PRC obtained funding in from the Centers for Disease Control for Participatory Action for Healthy Lifestyles PAHL , a 3-year qualitative research study to examine participatory processes in the dissemination of the Pathways intervention at three levels regional, state, and local using a community-based participatory research CBPR approach.
The idea was that increasing the level of community participation in the process of disseminating Pathways would increase implementation.
Health Promotion and Disease Prevention Theories and Models - Rural Toolkit
The objective of the project was to document the process through which evidence-based research findings were utilized by schools, public health professionals, agencies, the communities of study, and by other systems. Researchers at the UNM PRC who had been involved in Pathways were interested in sharing the curriculum developed in Pathways and studying the process of dissemination and utilization. However, as discussed below, developing a realistic design for incorporating participation required evolution of the structure of relationships between supporting institutions.
Individual schools, teachers, and school staff were intended users of the Pathways curriculum. DOH connected resources to potential community users through the institutional infrastructure of the state health apparatus.
Bestselling Series
The participatory framework of PAHL was to provide for integration of users, technical assistance, and connection to resources through active engagement and involvement of all partners in the process and with the creation of the SP Team. The SP Team concept, as defined in PAHL, was based on an approach commonly used in participatory research to create an explicit structure for local stakeholders to contribute to project planning and project design. As Wallerstein and Duran recommend, community participation generally requires the development of a specific structure, forum, or organization e.
However, in the specific context of PAHL, although the concept of the SP Team would have provided a formal, concrete mechanism for engaging community members and for integrating the work, realities on the ground conflicted with participation requiring ongoing coordination and time commitment from multiple stakeholders.
Accounting for the needs of community members and research partners required that PAHL develop less structured mechanisms to allow for community participation. As a result, rather than working via the SP Team, a PAHL project coordinator was hired to solicit input and guidance for disseminating and implementing the Pathways curriculum in different local contexts from individual schools. The PAHL project coordinator worked collaboratively with DOH to conduct presentations to potential adopters, and to identify interested schools and individuals.
Connections were built with opinion leaders, including teachers and school staff, community health representatives, tribal leaders, and stakeholders from IHS. The dynamic nature of the translation process required all stakeholders to operate with a degree of flexibility that is often difficult to accommodate in the research process. Her responsibilities included the Coordinated Approach to Child Health CATCH program that provides teachers with a framework for incorporating nutrition education and physical activity into the classroom curriculum.
Based on statements from interviews conducted as part of PAHL, coordinating trainings and technical support for two separate, seemingly competing programs was a burden for DOH field coordinators in terms of time and effort. As a result, working through the DOH field coordinators to develop connections to schools to implement Pathways and to serve as research sites proved challenging.
In the end, the PAHL project coordinator recruited schools directly on an individual basis. Ultimately, five schools two Bureau of Indian Affairs schools and three public schools serving Pueblo students. DOH did provide a funding mechanism for engaging schools in the possibility of implementing Pathways. In itself, the agreement by DOH to leverage the existing funding process for CATCH to include Pathways represented a potentially major development towards institutionalizing Pathways as an option for American Indian schools in New Mexico in a permanent fashion beyond the period of the grant.
Connectivity provided by DOH at the systems level was an important factor in the successful dissemination of Pathways, but cultivation of more personal connections in the community shifted to a the PAHL project coordinator. In the fall of , three direct training sessions in the Pathways curriculum were conducted by the PAHL Research Team with 46 individuals representing the five participating schools. Participants were primarily classroom teachers, but also included PE teachers, food service staff, a health educator, an educational aide, a nurse, a recreational therapist, and a parent—teacher organization president.
The fluid structure and flexible roles of the principal stakeholders in PAHL supported and encouraged dissemination of the Pathways curriculum. This inter-digitation between systems and stakeholders highlights the complexity involved in prevention research, and demonstrates the fluid mechanisms that develop in real-world settings in the context of unique local conditions.
Health Promotion Theory (Understanding Public Health)
Following training sessions, the selection and training of Pathways champions, and site-specific train-the-trainer sessions provided by the Pathways champions at their schools, all of the schools involved in PAHL made positive changes. Four out of the-five schools indicated using parts of the curriculum component, three schools hosted family engagement events, two schools reported improvements to school food service policy, and three schools reported using exercise break box activities and modified American Indian games.
At the same time, a number of factors were identified in PAHL data as hindering more successful and intensive implementation of Pathways components. Some teachers indicated that they were not entirely clear on implementation and did not feel confident about their ability to implement and integrate Pathways into their classroom curriculum. In post-training evaluation documents, some who attended the training reported that they left with what was really a rather cursory understanding of the overall Pathways approach and developed skills at a mechanical rather than a conceptual level.
Part of the challenge seems to have been related to the design of Pathways as an efficacy trial with a conceptual framework. Pathways was developed as an intensive, in-depth RCT intervention using a sequential, integrated interaction with teachers in their classrooms over multiple years, supported by a significant investment of resources and provision of materials. This meant that although an entire conceptual framework underpins the Pathways curriculum, the transfer being accomplished in PAHL was not necessarily of the conceptual package, but of individual components.
Some members of the research team believe that the inability of trainings to convey the bigger conceptual framework weakened the capacity of teachers and staff to understand how to incorporate discrete components into the curriculum in a meaningful way. In addition, a more overt challenge recognized during the project by teachers and principals had to do with schedule limitations and competing priorities for classroom activities.
PAHL was predicated on the idea that following the training, and with technical support provided by the researchers, teachers would implement Pathways with fidelity into their existing school curriculum. PAHL interview data indicates that there was a perception among people who took the training that Pathways would require a great deal of time to implement and a significant effort on the part of the teacher.
Teachers had begun to face new demands on curriculum time such that anything that did not directly address preparation for standardized testing was increasingly being excluded from the school day. Not only had there begun to be a reduction of art and music in schools but also PE programming and recess were also being eroded. In this context, where even traditional cornerstones of the school day were being deleted in favor of expanding standards-based academic instruction, teachers expressed the opinion that they found it difficult to justify incorporating nutrition education and physical activity into the required curriculum.
As a result, PAHL data suggests that the actual implementation of Pathways tended to involve only a few specific activities that could be integrated without much effort or time such as exercise break activities. At schools where the principal made Pathways a priority, teachers were more likely to actively engage in implementing components in the classroom.
In all cases, however, it was a small core of staff who were the prime movers adopting the intervention. Many of those who attended the trainings were not actually committed to the ongoing process of implementation. The experience of PAHL demonstrates how teachers and schools actively exerted agency in the process.
Some merely did not use the curriculum following the trainings. Teachers inspired by the training but with little time in the instructional day were able to make select components of Pathways fit with the required daily routines in their classrooms. In this context, supportive principals and committed staff made implementation more likely.
Despite the challenges, interest in the Pathways conceptual framework continued to motivate researchers and people in the community, and to capture the attention of stakeholders at IHS who had been involved in the original Pathways intervention. While modifying the entire Pathways curriculum was not possible, there was interest in and infrastructure for developing the physical activity component.
At that time, it was increasingly being recognized that community settings offer potential opportunities for increasing levels of physical activity among community members Paez et al. The idea that it is important for lifestyle interventions to recognize the differences in skill and ability that affects people's levels of physical activity, especially as this relates to age and past life experiences and history, was of interest Meyer and Gullotta ; Malina ; Marcus et al. Stakeholders involved in the implementation of Pathways via PAHL contributed to the development of a modified set of activities better reflecting the interests and needs of the community.
2h - Principles and Practice of Health Promotion | Health Knowledge
At the same time, IHS emerged as a key player, able to support the process of modifying and adapting the intervention. The fact that users were now embedded in an institution interested in adopting Pathways components further influenced success described below in the next stage. The agency of stakeholders contributed to the capacity for community input to actively transform and adapt the original intervention to more completely meet community needs.
The partners agreed to develop the PAK concept despite lack of specific funding for the effort. In , participating IHS programs provided funding for individuals from each pilot site to attend a 3-day training. Thirty-five people from 11 teams attended the training, and over the following year, participated in monthly conference calls to discuss their experience implementing PAK and training others in their communities.
During the evaluation summit, the results reported to IHS by trainers were positive, with participants describing enthusiastic reception in their communities. The principal critique that emerged from the summit was that people found the binder format too cumbersome, and the train-the-trainer manual and PowerPoint overly complicated and academic.
The idea of creating a more convenient, self-contained format was proposed. Over the next year, these recommendations were integrated into a re-design of PAK as a toolkit with discrete, small, spiral-bound books contained within a box. Making Health Policy Kent Buse. Introduction to Epidemiology Ilona Carneiro. Issues in Public Health Fiona Sim. Controlling Communicable Disease Norman D.
Economic Evaluation Julia Fox-Rushby. Issues in Public Health Joceline Pomerleau. Health Promotion Theory Maggie Davies.
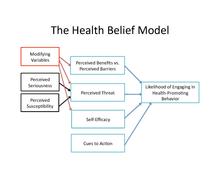
Medical Anthropology Robert Pool. Public Health in History Virginia Berridge. Managing Health Services Valerie Iles. Environmental Health Policy Megan Landon. Health Care Evaluation Sarah Smith. Understanding Health Services Nick Black. Conflict and Health Egbert Sondorp. Global Change and Health Kelley Lee. Environmental Epidemiology Megan Landon. Table of contents List of figures, tables and boxes List of authors Acknowledgements Overview of the bookSection 1: History and concepts of health promotion Chapter 1: As Nutbeam and Harris say, 'Changes in knowledge and beliefs will almost always form part of a comprehensive health promotion programme, and the health belief model provides an essential reference point in the development of messages'.
Behavioural intentions are determined by attitudes, the belief that the desired beneficial outcome will occur if a particular behaviour is followed; and by subjective norms, that is the person's beliefs about what other people think they should do normative beliefs. Later revisions of this model to the Theory of Planned Behaviour Fig 2.
The model thus predicts that a person is more likely to change behaviour if they believe the behaviour will improve their health, is socially desirable and there is social pressure to change, and that they feel they have personal control over the behaviour and the ability to change.
Self-efficacy is an important concept in social cognitive theory, it is concerned with self-judgements about how well one can execute courses of action, and can be very specific to individual behaviours. People avoid activities they believe exceed their coping capabilities, but they undertake and perform assuredly those that they judge themselves to be capable of managing' Bandura, This concept is indeed embodied in health promotion principles of empowerment and the Ottawa Charter definition of 'enabling people to take control of and improve their health'.
This model was developed by Prochaska and DiClemente to explain the process of behaviour change. It describes different stages of motivation to change behaviour and indicates the need for different processes of change to support movement between stages. Behaviour change is not seen as a result of a single cognitive decision, but a series of steps. Determination, or preparation ; the stage at which a person makes a serious commitment to change.
Based on study of addictive behaviours it also recognises that individuals may relapse and go back round the cycle again, and also that attention needs to be paid to the processes of maintaining behaviour change. The Stages of Change Model Fig. By understanding an individual's motivation, or readiness, to change Rollnick et al, and applying behavioural techniques such as motivational interviewing that are appropriate to different stages, the practitioner can support an individual through a change process and understand why some people are more responsive than others to simple advice and support.
For health practitioners the model helps them to see if the patient wants to make a change in a specified behaviour, the barriers that may need to be removed to make and sustain a change, and the fact that relapse is not a failure but simply a stage in a longer-term process of change. The authors emphasise that practitioners should be aware of developments in the use of the model and that further refinement of processes of change and how they are operationalised in stage-matched interventions is needed.
Social Cognitive Theory also known as Social Learning Theory is valuable to health promotion practice in that it encompasses both the determinants of health and individual behaviours more comprehensively than other theories. It attempts to embrace the subtle and complex relationships between people and their environment, and the social and environmental influences on their actions. It builds on Bandura's work on self-efficacy and a greater awareness of the ways in which the environment shapes behaviour by making it more or less rewarding to behave in certain ways.
For example, in the absence of legislation about smoking, if non-smokers are sufficiently assertive about not smoking it becomes more likely that a smoker will modify their behaviour.
Rural Health Information Hub
Thus the social influence has impacted on the individual's choice. This 'reciprocal determinism' describes the continuous interaction of the individual, their behaviour and the environment, and shows that the modification of social norms is a powerful health promotion tool. Further, personal cognitive factors play an important part, through the ability to learn a behaviour-reward pattern by observing others observational learning , valuing the behaviours displayed by significant 'role models', and attributing positive 'expectancies' to the outcomes of for example avoiding smoking, or exercising more.
Thus as well as social influence, peer influences and role models are also significant factors to consider in planning health promotion interventions. The importance of self-efficacy in actually making behavioural changes is further recognised in this model, and both observational and participatory learning may be necessary to build up the knowledge and skills for developing the 'behavioural capabilities' for successful behaviour change. Bandura A Self-efficacy mechanism in human agency. American Psychologist 37 2: Bandura a Self-efficacy in changing societies. A practical guide to health promotion theories.
American Journal of Health Promotion 17 1: Skilful communication is an important part of the delivery of health information to both individuals and communities. As has been shown in the theories relating to individual health behaviour, the social influences operating within groups or communities of people are significant factors on their behaviour.
While individual consultations with health practitioners and other interactions form an important part of health promotion, the individual's ability and desire to respond to health messages is mediated by their social group influences. Health promotion often employs influencing strategies at a community level, through mass media campaigns, education in schools or community groups.
An understanding of the theoretical basis of communication to communities and to individuals is important for effective transmission of messages. However again, such strategies, while a fundamental part of health promotion, are best supported by other mechanisms such as structural and system supports. Motivational interviewing is an approach to behavioural counselling especially aimed at fostering the individual's desire to change.
Using the Stages of Change model the technique recognises that at different stages people are in a different frame of mind about the behaviour concerned and have different motivations to change. The key elements of motivational interviewing are presented below to indicate the types of skills that are helpful in supporting encouragement of motivation to change. Give clear and concrete feedback to the patient about his behaviour, motives and personal situation.